
A couple of weeks ago I had a tutorial with my specialist portfolio students on the subject of automated blood counts. While discussing flow cytometry we touched on the subject of dichroic mirrors. A dichroic mirror is a sheet of material which allows light of certain wavelengths to pass through, which reflecting light of other wavelengths.
The use of a dichroic mirror is crucial in the operation of the flow cytometer, but for our purposes it is sufficient that the mirror is there and that it reflects some light and allows other light to pass. During the tutorial I explained that it was operated by magical pixies, and left it at that.
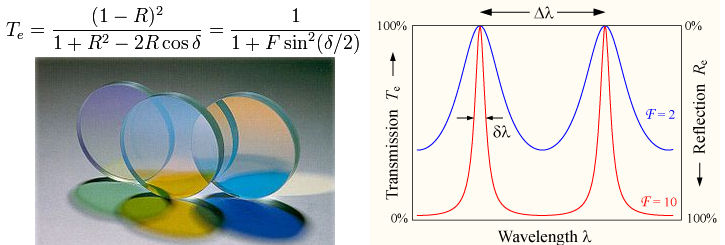
For some areas of science a biomedical scientist needs to know absolutely everything. However one cannot possibly be expected to know everything about everything. The physics of waves is something about which (up till now) I didn’t know very much. But some of my students have looked dichroic mirrors up. I now know that they operate by the principle of Fabry–Pérot interferometry.
It would seem (from wikipedia) that dichroic filters use the principle of thin-film interference, and produce colours in the same way as oil films on water. When light strikes an oil film at an angle, some of the light is reflected from the top surface of the oil, and some is reflected from the bottom surface where it is in contact with the water. Because the light reflecting from the bottom travels a slightly longer path, some light wavelengths are reinforced by this delay, while others tend to be cancelled, producing the colours seen.
In a dichroic mirror or filter, instead of using an oil film to produce the interference, alternating layers of optical coatings with different refractive indexes are built up upon a glass substrate. The interfaces between the layers of different refractive index produce phased reflections, selectively reinforcing certain wavelengths of light and interfering with other wavelengths. The layers are usually added by vacuum deposition.
By controlling the thickness and number of the layers, the frequency of the passband of the filter can be tuned and made as wide or narrow as desired. Because unwanted wavelengths are reflected rather than absorbed, dichroic filters do not absorb this unwanted energy during operation and so do not become nearly as hot as the equivalent conventional filter (which attempts to absorb all energy except for that in the passband).
Clear as mud?
For the purposes of counting blood cells it's probably good to know about interferometry in principle, but I don't pretend to understand it. I shall give the students a reference on the subject, but I for one will continue to describe a dichroic mirror as being operated by a magical pixie. And when assessing students I shall not expect any more explanation than that on the subject….













